Police use of force has arguably become one of the most visible public policy issues related to the criminal justice system in the United States today. Use-of-force issues surrounding acute behavioral emergencies and police restraint practices are currently dominating both the media headlines and research interests of major public policy shaping institutions. It is incumbent upon police chiefs to be prepared, understand the current issues, and examine their departments. Police leaders must proactively address the evolving medical, legal, and policy landscape surrounding restraint practices, including the growing controversy surrounding the term “excited delirium,” to ensure the safety of both officers and individuals in custody while upholding legal standards and fostering public trust.
The Naming Dilemma
Agitated, hyperactive, hyperadrenergic, or hyperagitated delirium are all medical terms describing the physiological state of a patient who is out of control, energized, incapable of stopping themselves, or unable to be redirected. In the past, it has been controversially called excited delirium syndrome, a medical diagnosis that is not accepted across many specialties of medicine, as it is not caused by a single condition.1
In the wake of major medical organizations disavowing the controversial and unproductive label “excited delirium,” professional police organizations have started adopting a range of new terms. These include medical behavioral emergencies (as used by the Police Executive Research Forum (PERF)), perceived unusual behavior (from the Institute for the Prevention of In-Custody Deaths), and acute behavioral disturbances or emergencies. To date, no consensus has emerged on a single term. Therefore, for the purpose of this article, the authors have chosen to use the term “acute behavioral emergencies,” in alignment with the IACP Center for Police Research and Policy.
The Excited Delirium Controversy
Widely regarded as a seminal document, the Physicians for Human Rights (PHR) report, “Excited Delirium” and Deaths in Police Custody (2022), conclusively states that excited delirium is a scientifically baseless and illegitimate medical diagnosis that has been misused to justify excessive force, rationalize preventable deaths, and impede police accountability in deaths in custody.2 This report has catalyzed extensive transformation within the medical, legal, and policing landscapes over the past four years. The report’s profound influence on legislative reforms and medical professional organizations necessitates that police chiefs thoroughly familiarize themselves with its assertions.
Following the report’s release, several major medical organizations notably reversed their long-held stances. For instance, the National Association of Medical Examiners (NAME) declared, “Although the terms ‘Excited Delirium’ or ‘Excited Delirium Syndrome’ have been used by forensic pathologists as a cause of death in the past, these terms are not endorsed by NAME.”3 Similarly, the American College of Emergency Physicians formally withdrew its support for their task force’s 2009 report on excited delirium.4
State governments have also responded to the PHR report and have taken action to restrict the use of “excited delirium” and related terms. California became the first U.S. state to ban the term as a cause of death and prohibit police officers from using it in incident reports.5 Colorado followed, not only banning its use in police reports and death certificates but also making it illegal for police agencies to train on or reference “excited delirium” or similar terms such as “agitated delirium” or “hyperactive delirium” in their training programs.6 Similarly, Minnesota has also prohibited “excited delirium” and similar terms in police training.7 Several other states are currently considering similar legislation.
“The phrase “I can’t breathe” must become more than a tragic plea; it must serve as a perpetual reminder of the need for this transformation.”
These policy reversals and legislative actions are tectonic shifts because they remove the medical legitimacy previously associated with “excited delirium,” profoundly impacting police legal defense and departmental liability. Police departments can no longer rely on it as a medically recognized cause of death or a justification for actions taken during critical incidents. This directly increases a department’s legal vulnerability in lawsuits stemming from in-custody deaths or injuries, and officers now face greater individual legal exposure as the absence of this medical explanation shifts the focus squarely onto their actions, tactics, and decisions while engaging individuals suffering acute behavioral emergencies.
This intensified scrutiny is highlighted by both recent academic publications and critical independent reviews. For example, a 2025 study, Mortality Classification for Deaths With Nonfirearm Force by Police, 2012–2021, directly concludes that the classification of cause and manner of death following nonfirearm force by U.S. police officers is inconsistent and often does not reflect or mention the use of force. This research, which analyzed data predating the major medical disavowals, is drawing attention to the accuracy of death attribution where police force is involved and the profound implications for public health data, legal outcomes, and police accountability. The study also revealed that, historically, only a small fraction (28.5 percent) of such deaths were classified as homicides, yet it highlighted a rise from 25.0 percent in 2012–2014 to 32.2 percent in 2018–2021.8 This is further exemplified by an independent audit of the Maryland Office of the Chief Medical Examiner’s (OCME) practices in May 2025, which found significant misclassifications and concluded that 36 deaths in police custody previously ruled undetermined, accidental, or natural should have been classified as homicides. The audit specifically identified patterns of racial bias and pro-law enforcement bias in past determinations and explicitly recommended that the Maryland OCME stop using “excited delirium” as a diagnosis.9 This sustained and increasing attention to the presumption of police intervention as the causation of death opens the door to more frequent homicide classifications, liability, and potential prosecution. The ground has shifted permanently, demanding strong executive leadership and rock-solid officer training.
Judicial Decisions to Know
Further complicating matters is a flurry of rapidly evolving judicial decisions involving restraint. Among the most significant is Scott v. Smith, a case involving the Las Vegas, Nevada, Metropolitan Police Department. In 2024 the Ninth U.S. Circuit Court of Appeals initially ruled that the officers were not entitled to qualified immunity. Crucially, the court found that the application of bodyweight compression to a prone individual during an acute behavioral emergency constituted deadly force, citing its potential to cause compression asphyxia and deeming it unconstitutional under the circumstances presented.10 However, in April 2026, the U.S. Supreme Court intervened, vacating the Ninth Circuit’s judgment and remanding the case for further consideration regarding the application of qualified immunity standards. Despite this procedural reset, the underlying legal vulnerabilities remain highly relevant.
Adding to this evolving judicial landscape, the Tenth U.S. Circuit Court of Appeals, in its June 2025 decision in Marquan Teetz v. Jason Stepien, further reinforced the severe legal risks regarding prone restraint. In a case involving a juvenile experiencing a mental health crisis who died in custody, the court affirmed that it was “clearly established law that applying pressure to a suspect’s back while in a prone position after being subdued is unconstitutional due to the significant risk of asphyxiation and death.”11 This ruling, from a different circuit, signals a potential judicial consensus on the dangers of prolonged prone restraint after subduing a subject and the heightened scrutiny applied to such force, especially when dealing with individuals experiencing acute behavioral emergencies.
While the ultimate disposition of the Scott case returns to the lower courts, police chiefs in all jurisdictions should take note. In the current legal and social environment, where there is intense scrutiny on police actions, prosecutors seeking to charge officers and plaintiff attorneys pursuing civil litigation will undoubtedly reference such clear and forceful determinations, regardless of circuit lines. These cases serve as a stark reminder that prolonged or excessive bodyweight on a subject can be deemed lethal and lead to severe legal consequences for both officers and their departments.
Chemical Restraint Issues
Adding further to the complexity, in most jurisdictions, emergency medical services (EMS) is often called to assess and transport people experiencing acute behavioral emergencies. They may have the option to administer chemically sedating medications, and while this intervention can be lifesaving when performed under the right circumstances, it is not without risk. Chemical sedation given early in an acute behavioral emergency can prevent escalation, a prolonged struggle, physical injuries to the individual and officers, and potentially death from severe acidosis. Chemical sedation given late in the course of a struggle may contribute to an already profound episode of acidosis and can lead to death if the individual’s condition is not recognized and immediately addressed.12 On balance, chemically sedating medications are far more likely to be helpful than harmful. A systematic review and meta-analysis of ketamine used for emergency sedation of agitated patients found 674 uses of ketamine that met the study criteria with only four deaths, two of which were unrelated to ketamine use and two of which were unlikely related to the ketamine use.13
Given the shifting legal landscape, which has led to criminal charges against both police and, more recently, EMS providers, police chiefs must clarify their agency’s role in these high-stakes situations. Departments should work with their responding EMS agencies to ensure there is a plan for care in behavioral emergencies, and patrol officers should be trained to engage with the medical responders to assure focus within their area of expertise. Police officers must avoid offering an opinion on the need for chemical restraint. Their focus should remain on securing the scene, relaying patient information, and facilitating a medical assessment by EMS to determine the appropriate treatment.
Professional Organizations Weigh In
Responding to these profound transformations, professional associations have begun releasing critical guidance and statements that police chiefs must review. In September 2024, for example, PERF released 15 Principles for Reducing the Risk of Restraint-Related Death.14 Concurrently, a joint consensus statement on collaboration between law enforcement and EMS during behavioral emergencies was issued by the National Association of EMS Physicians, the International Association of Fire Chiefs, and the IACP.15 Dialogue is ongoing, with the National Academy of Sciences having convened a study titled, Advancing the Field of Forensic Pathology: Lessons Learned from Death in Custody Investigations, with a report issued in October 2025.16
Prone Restraint: The Ongoing Debate and Evolving Science
Prone restraint is a common control mechanism for resistant subjects, utilized daily by police departments. Taking a combative subject to the ground for control is a foundational element in basic training academies and departmental defensive tactics curricula. Officers frequently encounter situations where the prone position is the only feasible alternative for control before and during handcuffing. This practical reality forms the fundamental basis of the amicus curiae briefs filed to the Supreme Court by organizations such as the National Police Association and the Police Officers Defense Coalition.17 Their core argument highlights the dilemma officers face: If standard police procedures for control, like prone restraint, are considered deadly force, this raises critical questions about viable alternatives for officers.
In support of their appeal to the Supreme Court, these organizations cite numerous research studies that find no inherent danger in the prone position itself. Indeed, some researchers argue there is no evidence to suggest that prone restraint, in and of itself, is inherently dangerous. For example, a significant 2015 study that prospectively examined 4,828 consecutive police use-of-force events across seven Canadian agencies, found that no subject died while in the prone position. This research concluded that prone restraint was not associated with an increased risk of sudden in-custody death, and that even in a worst-case scenario, 99.8 percent of subjects were expected to survive being in either prone or non-prone positions.18 Similarly, a 2016 prospective analysis examined 1,085 violent arrest incidents across 17 U.S. law enforcement jurisdictions also found no instances of sudden death and concluded that prone restraint was a safe method not associated with sudden in-custody death.19
Beyond Simple Restraint Positional Asphyxia or Metabolic Acidosis
Despite the research suggesting the inherent safety of prone restraint in isolation, the confluence of medical, legal, and operational factors in real-world incidents reveals a more complex and dangerous picture. Modern understanding points to specific physiological vulnerabilities that can turn a seemingly routine restraint into a fatal event.
A crucial 2025 review of the scientific literature by researchers Theodore Milner and Geoffrey Desmoulin, titled “Physiology and Biomechanics of Prone Restraint Respiration,” highlights these complexities. While acknowledging that a passive, calm individual in a prone position may not experience significant respiratory compromise, their analysis emphasizes that prior studies often failed to replicate the real-world conditions of an anxious, distressed, or intoxicated detainee who is struggling and being actively held down. Milner and Desmoulin conclude that hypercapnia (high carbon dioxide) is more likely to arise from the combined effects of multiple factors (such as struggling, obesity, anxiety, and drug intoxication), leading to metabolic acidosis that increases the risk of cardiac arrest.20 Their work provides the critical physiological underpinnings for why prone restraint in dynamic, high-stress situations may pose a heightened risk.
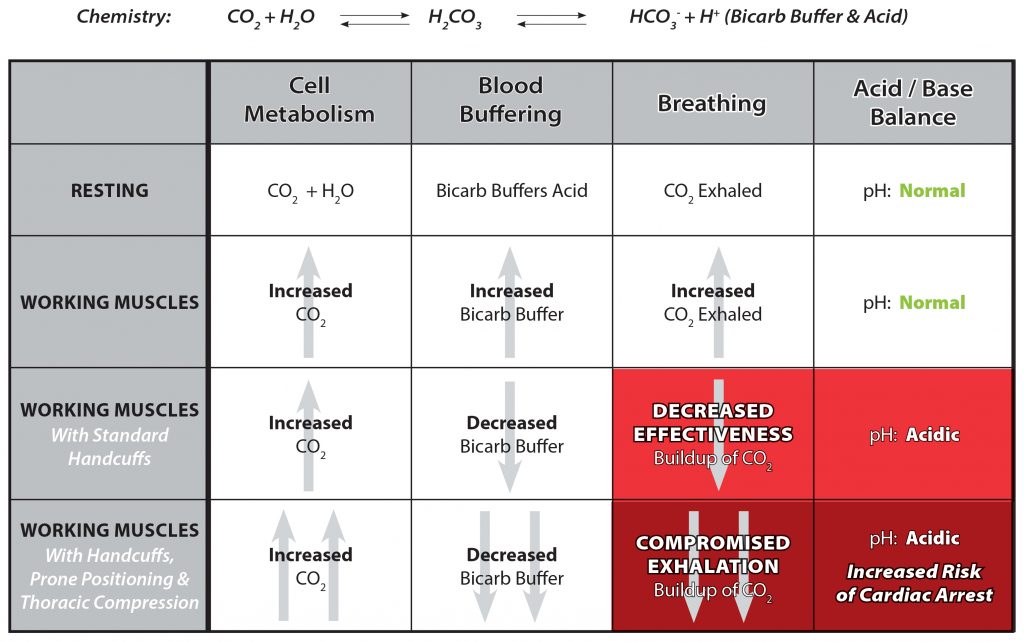
It is essential for police leaders to understand the medical nuances here. The courts often use the term “compression asphyxia” or “positional asphyxia,” but asphyxia is the inability to get oxygen in. Many medical experts believe that what may actually be occurring in these situations is a person’s inability to breathe out carbon dioxide, removing the ability of the body to maintain its acid-base balance through respiration. This physiological mechanism is more accurately described as profound combined acidosis. Intense struggle and muscle exertion create a dangerous buildup of acid in the blood, referred to as a metabolic acidosis. Normally the body buffers these acids by combining them with bicarbonate to form carbon dioxide, which can then be exhaled by rapid, deep breathing. If rapid, deep breathing is impaired, carbon dioxide levels will begin to climb and the metabolic acidosis will be combined with a respiratory acidosis. Thus, the prone position, particularly with sustained pressure, may not only prevent the body from compensating, but also may lead to increased acid production and, possibly, to a fatal cardiac arrest. This distinction between asphyxia and hypercapnia is critical and a central point of the ongoing scientific debate.
Recommendations for Adapting to the New Reality
Fostering a Unified Team Approach
A critical component of effective response to acute behavioral emergencies is a truly unified team approach. This is best articulated in the “Consensus Statement of the National Association of EMS Physicians, International Association of Fire Chiefs, and the International Association of Chiefs of Police: Best Practices for Collaboration Between Law Enforcement and Emergency Medical Services During Acute Behavioral Emergencies,” which explicitly advocates for a coordinated, pre-planned, and multidisciplinary approach among police, fire, and EMS, with appropriate medical oversight, to ensure the safest possible outcomes for individuals in crisis and the responders.21 However, in the authors’ experience during region-wide training on safe restraint practices, a profound lack of pre-planning and communication between police, fire, and EMS leaders is consistently observed. It is a fundamental duty of police executives to lead on this issue and bring together all stakeholders to develop a robust protocol that is in everyone’s best interest. The protocols developed in this working group should include three key principles:
- Prioritizing Medical Assessment: “Struggle Against Restraints = Medical Evaluation”
Police leaders and trainers should consider instilling a critical operating principle in their officers: “Struggle against restraints necessitates an immediate medical evaluation.” This concept is vital and has the potential for preventing in-custody deaths during acute behavioral emergencies. In the film Monty Python and the Holy Grail, the Black Knight continues to fight, even after he has lost his limbs.22 While the scene is comedic and hyperbolic, it demonstrates the dangers of disconnection from reality that occurs in some of the acute behavioral emergencies officers encounter.
When a subject or suspect continues to struggle after being restrained, especially following significant exertion or in a prone position, this behavior must be recognized as irrational delirium, a potential sign of severe physiological distress, not merely continued resistance. This sustained exertion, particularly under restraint, can rapidly lead to a dangerous buildup of acidic byproducts of metabolism, including lactic acid, that can result in a severe metabolic acidosis. Such a condition, particularly if combined with restricted breathing through positioning, if not promptly evaluated and addressed by medical personnel, could quickly escalate to cardiac arrest with tragic outcomes.
Teaching this principle through a primed recognition model with scenario-based training provides officers with a simple, actionable cue to identify a potential medical emergency, enabling them to call for and facilitate medical intervention without delay.
- Prioritizing Medical Assessment:“I Can’t Breathe = Medical Evaluation”
Building on the previous equation and continued prioritization of a medical assessment is when officers are faced with a subject stating, “I can’t breathe.” Some experts suggest that the statement made by a subject is less about the ability to breathe in and more about the ability to breathe out—in other words, their need to expel carbon dioxide. This concept is not only supported by real-world observations but is also validated by medical literature. A crucial article in the New England Journal of Medicine, titled “Handcuffs and Unexpected Deaths—‘I Can’t Breathe’ as a Medical Emergency,” explicitly makes this point, framing such declarations as a sign of a severe physiological crisis, not mere verbal resistance.23 Beyond this verbal cue of the restrained person, another critical sign is when the individual is observed to attempt to “lever” their chest off the ground in a “cobra pose,” lending further credibility to their plea. Just as with the “struggle against restraints” principle, this cue should be reinforced through scenario-based training, ensuring officers react automatically and appropriately in high-stress situations.
- Facilitatea Safe and Medically Sound Transport from Scene to Hospital
It is imperative that officers do not have to strategize about patient transport after a prolonged physical altercation. Instead, departments must develop robust, pre-planned guidelines in collaboration with EMS partners and medical oversight for seamlessly moving individuals from the scene of resistance to the ambulance and ultimately to the hospital.
Officers should be instructed to minimize the time a subject spends in the prone position. Guidelines should prioritize sitting the person upright or rolling them to their side once they are secured in handcuffs. An upright position is slightly preferred over a side-lying one, as continued contact with the ground, particularly along the ribs and upper torso, might subtly impede thoracic compliance (the chest’s ability to expand during breathing).
However, the critical challenge for departments—and a frequent gap in training—is providing officers with practical, safe methods to actually transition a still-resistive subject from the street into a stable position for ambulance transport. It is crucial to recognize that achieving optimal positioning can be difficult in dynamic situations, highlighting the importance of swift medical intervention once control is established. Every department must establish methods for secure and injury-reducing transfer. One possibility for agencies to consider is the use of a standard medical backboard.24
Conclusion
The landscape of police response to acute behavioral emergencies has irrevocably shifted. The confluence of evolving medical understanding, landmark legislative changes, judicial decisions, and heightened public scrutiny demands a proactive response from police leadership.
Police chiefs face a critical imperative to lead the transformation of their departments by embracing genuine inter-agency collaboration, instilling a “struggle against restraints = medical evaluation” principle in their training, and establishing clear, medically sound transport procedures. This is not merely about compliance with new legal and medical standards; it is about fundamentally reorienting police practice to prioritize life, protect officers from undue legal and departmental liability, and foster unwavering public trust. The phrase “I can’t breathe” must become more than a tragic plea; it must serve as a perpetual reminder of the need for this transformation.
Liability and public trust hinge on the demonstrable preparedness and efforts taken by the department. By acting decisively now, police leaders can take actions to navigate these complex challenges, significantly reduce the risk of tragedy, and solidify their agencies’ commitment to both officer safety and the well-being of the communities they serve in the era of 21st century policing. d
Notes:
1Gary M. Vilke et al., “Excited Delirium Syndrome (ExDS): Treatment Options and Considerations,” Journal of Forensic and Legal Medicine 19, no. 3 (2012): 117–21; American College of Emergency Physicians Hyperactive Delirium Task Force, ACEP Task Force Report on Hyperactive Delirium with Severe Agitation in Emergency Settings (2021).
2Brianna da Silva Bhatia et al., “Excited Delirium” and Deaths in Police Custody: The Deadly Impact of a Baseless Diagnosis (New York: Physicians for Human Rights, 2022).
3National Association of Medical Examiners, “Position Statement, Excited Delirium,” March 6, 2023.
4American College of Emergency Physicians, “ACEP Reaffirms Positions on Hyperactive Delirium,” news release, October 12, 2023.
5California Legislature, A.B. 360, Excited Delirium (2023) (passed).
6Colorado General Assembly. HB 24-1103, Concerning Prohibitions on the Official Use of the Term “Excited Delirium,” April 4, 2024.
7Minnesota Statutes, Training in Excited Delirium and Similar Terms Prohibited, § 626.8437 (2024).
8Justin Michael Feldman, Tracey Lloyd, and Phillip Atiba Solomon, “Mortality Classification for Deaths with Nonfirearm Force by Police, 2012–2021,” JAMA Network Open 8, no. 3 (2025): e252371.
9Jeff Kukucka et al., An Independent Audit of Restraint-Related Death Investigations at Maryland’s Office of the Chief Medical Examiner (OCME) from 2003-2019 (Baltimore, MD: Maryland Office of the Attorney General, 2025).
10Scott v. Smith, No. 23-15480 (9th Cir. 2023).
11Teetz v. Stepien, No. 24-3153 (10th Cir. 2025).
12Jonathan Smith, Melissa Costello, and Roberto Villaseñor, Investigation Report and Recommendations (City of Aurora, February 22, 2021).
13Natalie Sullivan et al., “Ketamine for Emergency Sedation of Agitated Patients: A Systematic Review and Meta-Analysis,” The American Journal of Emergency Medicine 38, no. 3 (2020): 655–61.
14Police Executive Research Forum (PERF), 15 Principles for Reducing the Risk of Restraint-Related Death (PERF, 2024).
15Michael K. Levy et al., “Consensus Statement of the National Association of EMS Physicians, International Association of Fire Chiefs, and the International Association of Chiefs of Police: Best Practices for Collaboration Between Law Enforcement and Emergency Medical Services During Acute Behavioral Emergencies,” Prehospital Emergency Care 28, no. 8 (2024): 1–7.
16National Academies of Sciences, Engineering, and Medicine, Strengthening the U.S. Medicolegal Death Investigation System: Lessons from Deaths in Custody (National Academies Press, 2025).
17Brief of Amici Curiae of the National Police Association and the Police Officers’ Defense Coalition in Support of Petitioners, Smith v. Scott, No. 24-1099, Petition for Cert. to 9th Cir. (2025).
18Christine Hall et al., “Restraint in Police Use of Force Events: Examining Sudden In Custody Death for Prone and Not-Prone Positions,” Journal of Forensic and Legal Medicine 31 (2015): 29–35.
19Darrell L. Ross and Michael H. Hazlett, “A Prospective Analysis of the Outcomes of Violent Prone Restraint Incidents in Policing,” Forensic Research & Criminology International Journal 2, no. 1 (2016): 16–24.
20Theodore E. Milner and Geoffrey T. Desmoulin, “Physiology and Biomechanics of Prone Restraint Respiration,” Medicine, Science and the Law 65, no.4 (2025): 311–20.
21Levy et al., “Consensus Statement of the National Association of EMS Physicians, International Association of Fire Chiefs, and the International Association of Chiefs of Police.”
22Monty Python and the Holy Grail, scene “Black Knight,” dir. Terry Jones and Terry Gilliam (Python (Monty) Pictures, 1975).
23Matt Bivens, Eric Jaeger, and Victor Weedn, “Handcuffs and Unexpected Deaths—’I Can’t Breathe’ as a Medical Emergency,” New England Journal of Medicine 391, no. 22 (2024): 2068–9.
24James J. Gerace and Michael W. Dailey, “Police Practice: Safe Restraint of Agitated Patients,” FBI Law Enforcement Bulletin, January 10, 2023.
Please cite as
James Gerace et al., “Leading at the Intersection of Crisis and Care: Acute Behavioral Emergencies and Modern Restraint Dilemmas,” Police Chief Online, June 3, 2026.